On the 17th January 2017, I interviewed the documentary filmmaker Paul Berczeller, who has made a documentary for Channel 4 about the origins of Donald Trump, going back to his grandfather who emigrated from Germany and ran brothels for gold miners in the Old West.
I talked to him about what had to happen to create a Donald Trump, and to get his perspective on the reality of a Trump presidency.
Paul’s film ‘Meet the Trumps’ is available to watch on All4 here.
This interview was initially recorded for iRadio Coventry, and aired on 17/01/2017.
This is the result of a very regrettable campaign of misinformation by the BMA over the Summer that’s tried to scare doctors about these proposals, suggesting that they’re going to have big pay cuts. I would urge every doctor before they participate in this strike to actually look at the government’s offer: we are bringing down weekend rates in order to improve cover at weekends, but we’re increasing basic pay by around 11%.
In a web worthy of the most hardened conspiracy theorist, the Right Honourable MP has positioned himself as the spider, trying to hold the strands together against the onslaught of brainwashed BMA flies flying towards it. “Don’t worry, I won’t suck the life out of the health service,” he seems to say, “I won’t be cutting your pay, I will just be readjusting how it is delivered into a format that I find preferable. Oh, the professionals don’t agree? They’ve found that none of what I am saying adds up? They must be out to get me.”
Jeremy Hunt has also rejected any notion of conciliatory talks through the Advisory, Conciliation and Arbitration Service (ACAS), saying that his ‘door has been open for talks since June, and the BMA have refused to engage at any stage with talks’. He tweeted recently that any pre-conditions that the BMA are referring to are completely fabricated, even having the gall to post a link to the letters to the Junior Doctor’s Committee (JDC) Chair in which the preconditions are described.
Back on the 4th November, the JDC Chair Dr Johann Malawana released a statement saying that:
To get back around the negotiating table we have repeatedly called on the government to remove the threat of imposition and provide us with concrete assurances on a safe and fair contract. Today’s announcement falls short on both counts as, once again, the headlines do not match up to reality.
Crucially, the proposals fail to deliver safeguards with real teeth to protect safe working patterns and, with it, patient and doctor safety. Furthermore, the proposals on pay, not for the first time, appear to be misleading. The increase in basic pay would be offset by changes to pay for unsocial hours – devaluing the vital work junior doctors do at evenings and weekends. While, in the short-term, existing junior doctors may have their pay protected, protections will only exist for a limited time.
So, there were preconditions to the contract negotiations, including an imposition of the terms regarding pay, which I might again emphasise are laid out in the letters Mr Hunt posted online.
So, despite Mr Hunt’s insistences, there would be substantial effects on doctor’s pay.
So, it’s not all about pay in the first place, there are genuine concerns about the risks placed on patient safety by the new contract.
And he wonders why doctors have exactly zero trust in him?
I would prefer to give him the benefit of the doubt on this one. All of the evidence points towards a campaign of misinformation, not on the part of the JDC, but rather orchestrated by Jeremy Hunt and the Department of Health. This would all seem to indicate he is being wilfully dishonest; however, I suggest another option.
He genuinely believes everything he is saying, and he genuinely believes that the backlash given to him at every turn over his policies from people in the know is simply because he is poor old Jeremy Hunt, just trying to make the world better. In simpler terms, he is delusional, to the point where it is interfering with his job. He is caught up in the collective Tory delusion that by implementing private sector business practice everywhere, the country can be saved- even when it is demonstrably not working, it is just an element of militant doctors or left-wing malcontents trying to stir up trouble.
In response to Jeremy Hunt rejecting talks through ACAS, the BMA have released the following statement:
It is clear that trust has broken down between junior doctors and the government, which is why we are offering conciliatory talks via ACAS. If it is true that Jeremy Hunt has refused our offer, all he is doing is entrenching himself even further.
This is not just one or two junior doctors who believe that his proposals are unsafe for patients and unfair for doctors. The fact that today’s ballot result is near unanimous should be a wake-up call for the government. Instead of continuing to ignore the views of tens of thousands of junior doctors who, in the health secretary’s own words, are the backbone of the NHS, he should, if he really wants to avoid industrial action, accept the BMA’s offer of conciliatory talks.
One can only hope that even the upper echelons of the Tory party must eventually take note of the catastrophic failures in the Department of Health, and reshuffle accordingly.
But it’s entirely possible that they are all delusional too.
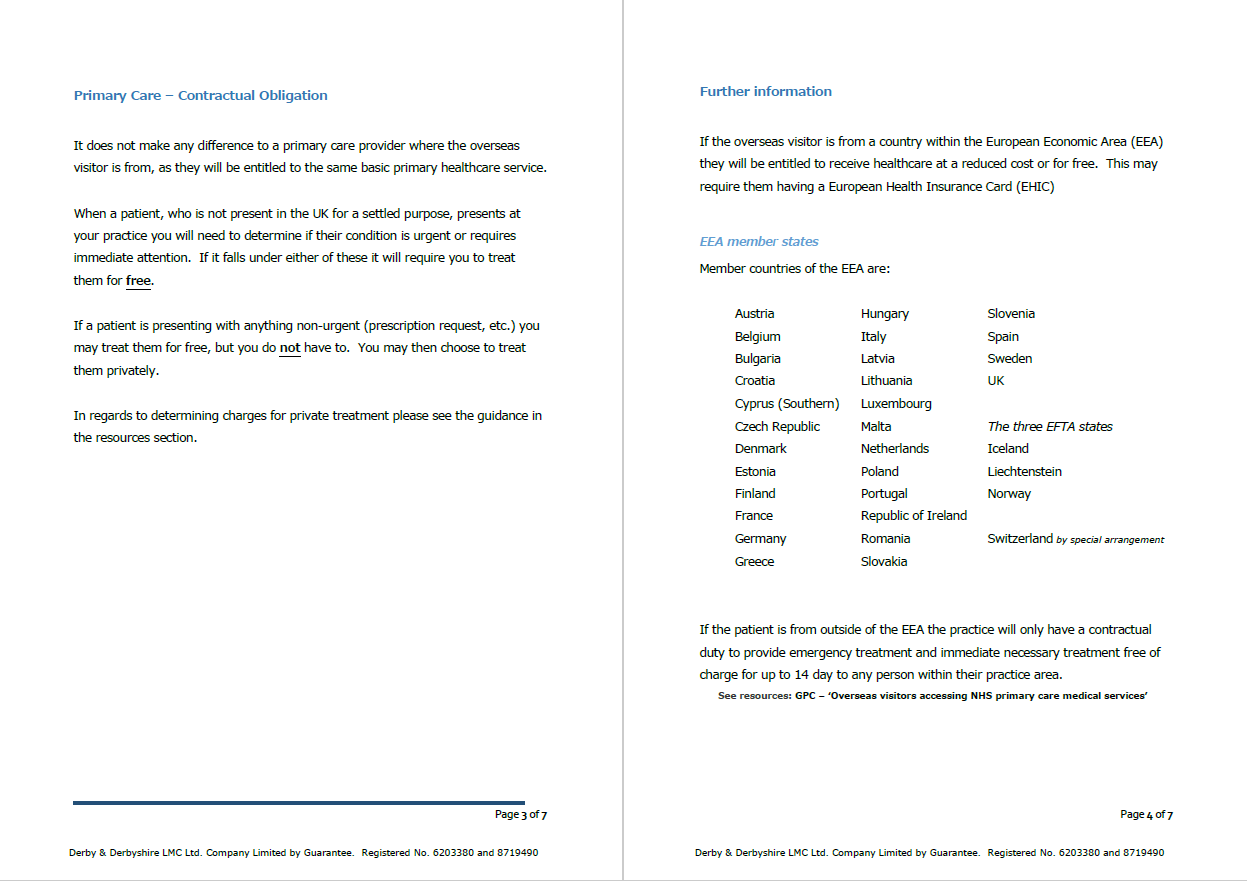
Derby & Derbyshire LMC guidance from August 2014 on charging overseas visitors, demonstrating how much the re-interpretation from the BMA has affected the practicalities of providing care for non-UK residents. Source: Derby & Derbyshire LMC
Up until now, the general consensus among GPs seems to have been that it was up to the discretion of the practice to decide whether or not to charge for treatment of anything non-urgent to overseas visitors. A Derby & Derbyshire LMC guidance pamphlet on ‘Overseas Visitors’ from August 2014 also makes clear that any patient from outside of the EEA (European Economic Area) was only entitled to emergency treatment and immediate necessary treatment free of charge for up to 14 days. Under the new guidance however, anyone, ‘regardless of nationality and residential status may register and consult with a GP without charge’.
The rewording of the guidelines has, despite the BMA’s assurances, completely changed their practical effect. One of the most worrying potential effects is to increase health tourism to the UK. This could potentially lead to yet another drain on the NHS’s dwindling financial resources, as people from outside of the EEA will effectively be paying nothing in the way of taxes or health insurance for the services provided. There are already procedures in effect to make sure that anyone in urgent need of healthcare, regardless of where they are from, will be able to get it through the NHS.
In response to this particular issue however, they have said that ‘international visitors are welcome to use the NHS provided they pay for it- just as families in the UK do through their taxes’, while also saying that they have a ‘long standing commitment not to charge patients directly for GP or nurse consultations’. The reason being, according to a Department of Health spokesperson, that keeping these services free is in the public interest as someone with a serious infectious illness like TB or Ebola might be ‘deterred from seeking treatment because they fear being charged’.
One can’t help but think that if a patient had Ebola (a horrific disease infamous for its tendency to cause bleeding from every orifice) that it would classify as emergency care requiring urgent treatment, and the patient probably wouldn’t be thinking of calmly booking an appointment with their GP, nor would they be tremendously worried about any sort of ‘charges’.
It should be noted that there are procedures in place to protect the vulnerable in the UK; asylum seekers and refugees are already entitled to treatment. Another overseas visitors guidance document produced by the GPC from May 2005 said that in the event that a patient is not eligible for free treatment and is unable to pay privately, they should be referred to The Refugee Council for assistance. It also notes a resolution passed at the LMC conference in 2004 ‘which opposed proposals to deny failed asylum seekers free primary medical services’.
It seems somewhat apparent, then, that all the bases for vulnerable non-UK and -EU residents seeking NHS treatment were already covered. This makes the new reinterpretations of the guidelines all the more perplexing.
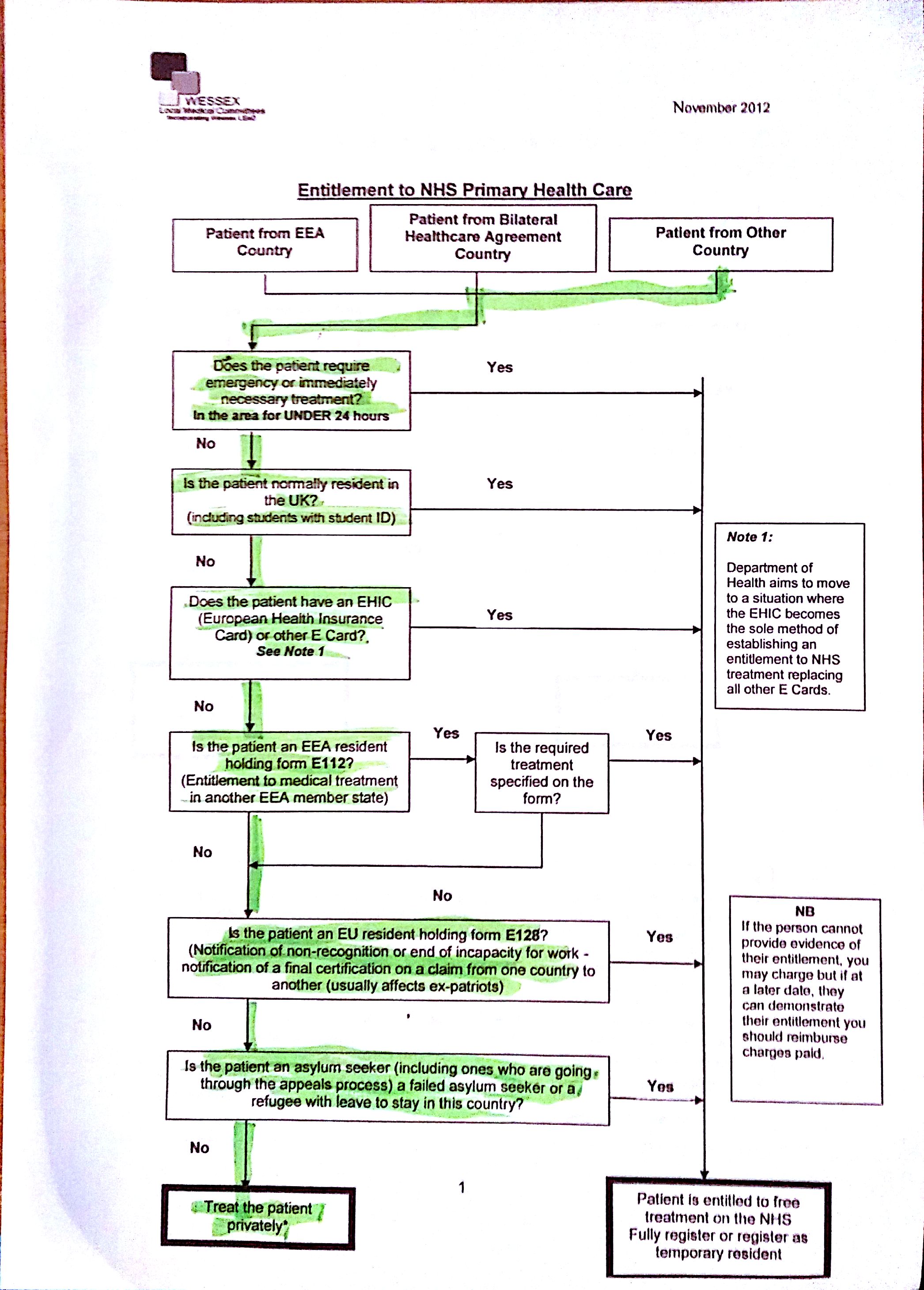
A flowchart distributed by Wessex LMC in November 2012 indicates that previously, primary care for non-UK residents outside of a particular set of circumstances would be delivered privately, unless the patient was ‘residing in the country for 3 months or more for a settled purpose’. Source: Wessex LMC
The NHS is not a charity. It is a taxpayer-funded health service. The money to treat patients doesn’t condense from the air like droplets in a glass bottle; it has to be trickled in from the general public and (theoretically at least) responsibly distributed to where it is needed. EEA residents also fund our NHS when they need treatment, through medical insurance cards and their own taxpayer’s money. In addition to this, a survey conducted by PULSE shows that 77% of GPs support the government’s efforts to stop health tourism by charging foreign visitors for accessing primary care.
These new guidelines leave the NHS wide open to exploitation from health tourists seeking a cheap diagnosis and course of treatment. Dr Zishyan Syed, a GP in Kent, has said:
It is a sad reality but there is abuse of the NHS by foreign visitors. It is only fair that they pay upfront if they are not entitled to free care on the NHS. The NHS is in trouble and it is only right that the Government stops anyone from taking advantage of a system that is already under immense pressure.
It would be wonderful if the NHS could treat everyone in the world for free, but the realpolitik of the situation is that they cannot afford to. At this time, it is somewhat reckless for the BMA to reinterpret the guidelines in this way; although they are just following Government regulation. It is more damning that this has been done in the name of the Department of Health
Amendments: Title and other elements have been amended to more accurately reflect the story.
NHS England have since made contact. Their spokesperson has said:
There’s various things going on that have perhaps caused a bit of confusion. DH are looking into guidance around charging people from abroad.
All that we’re doing is just reconfirming the existing guidance around registration for patients. There has been a bit of confusion in some practices about asking for documents to prove that they were local or ordinarily resident, which isn’t required for primary care.
So we’re just reiterating new guidance, there’s nothing new in there.
There is a lot of confusion with word also going around that DH is considering charging for secondary or hospital treatment.
The BMA has issued a warning that students from deprived areas in the country may be ‘held back from a career in medicine’, because most medical schools require a GCSE in Triple Science in order to apply. This award was found not to be offered as often in deprived areas, and when it is offered, lower numbers of students applied for it. The BMA have called for all secondary schools to offer Triple Science as a course, for medical schools to consider contextual data (like details about the applicant’s school or where they live) in their admissions, and also for outreach schemes between medical schools and secondary schools to spot possible talent early on.
The Beveridge Report was published in 1942, and laid the basis of the push for social welfare and greater social mobility in post-war Britain. It proposed support ‘from cradle to grave’. Source: Wikipedia
I must admit, I don’t remember my own Triple Science classes being that under-subscribed. I went to school in the Warwickshire town of Nuneaton. Nine areas in Nuneaton are featured in the 10% most deprived communities in the country, according to a report from Warwickshire Observatory from 24th March, 2015. For clarification, I don’t live in any of those nine areas, and I would not refer to myself as deprived by any stretch; however many of the people from my school came from these areas. Students at Higham Lane School (which I attended 2005-2010) were- and still are, as far as I know- offered the chance to do the Triple Science GCSE. Several people I know from school have gone on to medical schools and are currently in training to be doctors, although I would estimate that most of these people did come from middle-class households.
Higham Lane School’s website says that they are amongst the top 100 performing non-selective state schools in the UK. Source: Higham Lane School
That disclaimer aside, it is important to remember that one anecdotal case does not a rule make. The BMA’s report, ‘The Right Mix: how the medical profession is diversifying its workforce’, found that in the areas of Hull and Newcastle, less than 65% of schools offer the Triple Science course. In Newcastle, only around one in five students were taking the course (18%); in Hull, this was significantly lower, at around one in ten (11.4%). Compare this to Rutland, an area significantly more well-off than those mentioned, in which over a third of students (36.2%) study the subject, which is taught at all schools in the area. 80% of applicants to medical qualifications in the UK come from 20% of the schools, so one must cross their fingers and hope that the next Sir Alexander Fleming hasn’t had the misfortune to be born in Hull (sorry, Hull).
A possible problem is the perception of medical schools by people of lower socioeconomic class. A 2004 study published in the BMJ and co-authored by Professor Trisha Greenhalgh found that opinions of medical school didn’t change much when considered by gender (over half of medical students in 2013 were female) or by ethnicity. Class on the other hand had a significant effect:
Pupils from lower socioeconomic groups held stereotyped and superficial perceptions of doctors, saw medical school as culturally alien and geared towards “posh” students, and greatly underestimated their own chances of gaining a place and staying the course. […] Pupils from affluent backgrounds saw medicine as one of a menu of challenging career options with intrinsic rewards[.]
The study also found that while both groups were concerned about the costs of study, only the poorer pupils saw it as a factor of constraint.
There is a clear and obvious problem in the country today with the perception of the medical profession. With the current crises of under-staffing in hospitals across the country, it is also a potential time-bomb for the NHS. The recent furore over junior doctors and their salary cuts, along with Jeremy Hunt’s push for an ill-planned 24/7 NHS (as many infuriated medical staff have already pointed out, doctors already work weekends) will likely turn people off the profession, especially potential future doctors from lower socioeconomic backgrounds who, even back in 2004 according to the Greenhalgh study, already considered the profession to require ‘prohibitive personal sacrifices’.
A push needs to be made to attract as many people to the profession as possible from all backgrounds. An anti-propaganda campaign to the Tories’ poisonous rhetoric and restrictive policies towards the poorer community’s ability to study needs to be orchestrated. As well as this (as the BMA rightly says), there needs to be a effort to make these opportunities available and viable for everyone. This involves being outraged by the fact that many students can no longer afford their own rent while studying; this includes providing as much support for reforming the student loan system as possible; this means providing an information campaign directed at pupils in deprived areas to educate them that careers in medicine are in reach, that they are attainable with hard work and dedication, and that the rewards from such endeavours stretch far wider than just financial incentives.
It’s saving lives, at the end of the day, in the most literal sense.
We all get advertising calls. Our phone numbers are constantly being sold off to marketing agencies, leading to those persistent calls asking about our accidents and PPI claims which don’t seem to stop, even when we follow the prompt to “press 9 to opt out”. They tend to remain in the part of our lives marked annoyance, rather than being seen as anything more malign- most of these companies don’t even know the names of the people they are calling, only their numbers. However, recent developments suggest that the line may be getting blurred.
On the 20th October, the Information Commissioner’s Office concluded an investigation into Pharmacy2U, an NHS-approved prescription-delivery service that has now been fined £130,000 after it was found that they had been selling patient details to advertising agencies. The incident was originally uncovered by a Daily Mail investigation. Pharmacy2U is registered with both the General Pharmaceutical Council and the Care Quality Commission. The company delivers repeat prescriptions to patients who might be unable to collect the drugs in person.
Pharmacy2U are not currently being subjected to punitive measures for their breach of patient information to marketing agencies. Source: MORE 4ME
On their databases, by necessity, they have a lot of private information about the patients they supply, including names, ages, genders, home addresses, contact details and (and here’s the part where you should feel a chill crawling up your spine) their prescriptions, from which one could reasonably infer what maladies they are suffering from. I should make it clear, that I have found no reason to believe that specific medical details were given out as a part of these information packages to the marketing agencies, however according to the ICO report, likely conditions were advertised, and ‘selections were available based on age, sex and how recently the customer had used the service.’
In the United Kingdom, there are laws against the marketing of the public’s private information without their consent. The Data Protection Act of 1998, along with the Privacy and Electronic Communications Regulations, 2003, make it so that for a company to sell information about one of their users/customers/clients/etc., they must first have their consent. The 2003 regulations made it so that positive consent was required online, which translates to an oft-overlooked tick box in which you are signing over to the company the ability to do share your details with their “carefully selected marketing agencies”.
Bear in mind that one of Pharmacy2U’s carefully selected marketing agencies (Health Marketing Ltd.) was under investigation by the Advertising Standards Agency for printing misleading information about Glucosamine supplements. The ICO have noted that, due to there being no publicly available information about this investigation at the time, Pharmacy2U were most likely unaware of this particular agency’s disrepute.
This does not excuse them, not by an absolute mile- despite their protests otherwise, the act of a trusted and reputable company selling patient information to any kind of marketing company, especially when many of the patients due to their age may not have been internet-literate enough to notice those infernal tick boxes, is abhorrent and highly cynical.
An apology and a £130,000 fine seem like water balloons against a well-armoured tank. Patient details were sold in lots of 1,000 for £130 apiece (13p per data set). Around 21,500 patient’s details were sold, although 100,000 data sets were advertised. The fine seems to be in direct relation to the total amount of revenue that could have been made from the sales of this data. Surely then, this is not a fair sentence?
The BMA are unhappy with the current measures being taken against Pharmacy2U by the ICO. Source: Wikipedia
If a thief were to steal a locket of immense emotional importance to its rightful owner, then the public would be outraged if when the thief was caught he was asked only to return the item and have done with it. The details released were as valuable to Pharmacy2U’s clients as to the hypothetical victim’s jewellery above: they constituted a significant part of their identities, leaving them open to specific appeals made using potentially very sensitive information.
The BMA have made a statement much to this effect. They note that the report raises ‘serious concerns’ about Pharmacy2U’s ability to handle data in a proper and secure manner. They go on to say:
Although the BMA welcomes the information from the ICO investigation, we are pushing for custodial penalties for those who wilfully or recklessly abuse personal data. In our view, the current financial penalties do not offer enough of a deterrent.
Source: BMA
The EMIS Group, a minority shareholder in Pharmacy2U, have made it clear that they were unaware of the company’s activities. They also confirm that Pharmacy2U is ‘no longer [selling] customer data and moving to a proactive consent model for its own marketing’ and that they did not contravene the DPA deliberately, nor were they properly informed at the time of their decision that some of the marketing companies may have been ‘involved in fraudulent activity’.
Corrections: I have been informed by Pharmacy2U’s PR representatives that the number quoted for data leaks was wrong; it is in fact 21,500 data sets that were released, not 100,000. I originally misread this figure from the BBC News website, although did not check closer as it referred to the total amount of data advertised.
I would also like to make it clear that EMIS Group is a minority shareholder in Pharmacy2U, Pharmacy2U is not a subsidiary of EMIS.
Additions: In reviewing the ICO’s report after receiving this information, I have also found that the data card used to advertise the data ‘included an age breakdown and a list of health conditions that customers were likely to suffer from’, which while not specifying which customer had which condition, but they were advertised with such information as ‘age, sex and how recently the customer had used the service’. This is an important point, as I had previously been unaware that any medical information at all was presented during the sales.
I adapted the name of this blog, “Cut For Stone”, from a line of the original Hippocratic oath made between the 5th and 3rd century BCE. It was devised by the physician Hippocrates for medical students under his tuition, as a means of ensuring potential physicians maintained an ethical manner and upheld their obligations. An abridged translation of the original line is as follows:
I will not cut persons labouring under the stone, but will leave this to be done by the [surgeons]
The stone in reference is likely to be kidney stones or something similar. It is well known that surgery is a somewhat precise and, in unskilled hands, dangerous art; this part of the oath appears to encourage a humility in these early doctors. “If you do not know how,” Hippocrates seems to say, “then ask someone who does to help”. This, to me, is a good central stone by which to base this blog.
A Byzantine manuscript of the Hippocratic Oath, 12th Century ACE. Image Source: Wikipedia
Again and again, we have seen officials blindly altering legislation without any heed to the words of experts speaking against it- as I write this, here in the UK, the Department of Work and Pensions is being looked into for their treatment of the disabled, and the Tory cabinet are dismissive that anything is wrong. Jeremy Hunt MP, in his tenure as the Secretary of State for Health, has faced widespread staff shortages and NHS budget deficits of potentially over £2.5 billion leading to a difficulty to maintain a proper quality of care. Recently, he made an announcement to insinuate that it was not he, but the BMA that was misleading junior doctors who had worked out that they were heading towards a substantial pay decrease.
I fully believe that these people are working with what they consider the country’s best interests at heart. Unfortunately, in their eagerness to sell the UK off to the private sector piece by piece, they have failed to consider fully the impact of their measures in the world of reality, not ideology. Using disreputable companies like ATOS to decide whether or not those in need are truly needy enough, and cutting tax credits away as if they were so much unneeded fat has created the circumstances which have led to widespread anguish, financial difficulties and in some cases, even death.
The NHS is one of the hardest-hit public services by government reforms. Image Source: Wikipedia
It could all have been avoided; it is currently almost being ignored- hidden, if you consider the changing of the definition of child poverty by Iain Duncan Smith as any indication. If only these people, in their pursuit of the “stone” in our society, had considered asking first where the stone was located, and exactly how one breaches a kidney like the NHS without harming it. Proper, evidence-based policies, taken fully into consideration and not rejected with derision, might have led to true success.
I believe the way to incite change is through transparency. Transparency puts pressure on those in power by laying bare their actions, that they may be judged by a jury larger than themselves. That is the purpose of this blog.
This post will in future take the function of a manifesto. I intend to write this blog with the following directives in mind:
This blog will be for the purposes of news and analysis of current events within the UK.
The NHS is one of our most treasured assets, and it must be protected for the future prosperity of our country.
My writing will be clear, informed and current.
I write in order to aid transparency in the opaque parts of the public and political spheres.
I will try to the best of my abilities to put the needs of those in need first.
It is possible to be wrong, and sometimes necessary in the search of improvement.
I am opposed to the privatisation of public assets where it is demonstrated to put them at risk and/or to have a negative effect on the country.
Thank you for reading. First updates will be along as soon as possible.